
Abstract
Background
Hospital volume is known to be a crucial factor in reducing postoperative morbidity and mortality in laparoscopic gastrectomy for gastric cancer. However, it is unclear whether surgeon’s individual experience can overcome the effect of hospital volume.
Methods
Clinicopathologic data of initial 50 laparoscopic gastrectomy cases were collected from six gastric cancer surgeons. Half of the six surgeons worked in high-volume centers, and the other half worked in low-volume hospitals. Perioperative outcomes were compared between the high-volume centers and the low-volume hospitals.
Results
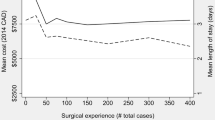
Three low-volume hospitals in this study contained significantly more male and older patients with a higher American Society of Anesthesiologists score than high-volume centers. Although high- and low-volume hospitals mainly used laparoscopy-assisted and totally laparoscopic approach, respectively, there were no differences between the two groups in the extent of resection, operating time, estimated blood loss, and number of collected lymph nodes. Postoperative recovery such as duration to soft diet and hospital stay did not differ between the high- and the low-volume hospitals. No significant difference was found in postoperative morbidities by Clavien–Dindo classification. There was no mortality reported in both groups of the enrolled hospitals.
Conclusions
Hospital volume is not a decisive factor in affecting postoperative morbidity and mortality for well-trained beginners in laparoscopic surgery for gastric cancer.

Similar content being viewed by others

References
Ecker BL, Datta J, McMillan MT, et al. Minimally invasive gastrectomy for gastric adenocarcinoma in the United States: utilization and short-term oncologic outcomes. J Surg Oncol. 2015;112:616–21.
Maduekwe UN, Yoon SS. An evidence-based review of the surgical treatment of gastric adenocarcinoma. J Gastrointest Surg. 2011;15:730–41.
Kim CH, Song KY, Park CH, Seo YJ, Park SM, Kim JJ. A comparison of outcomes of three reconstruction methods after laparoscopic distal gastrectomy. J Gastric Cancer. 2015;15:46–52.
Yoo CH, Kim HO, Hwang SI, Son BH, Shin JH, Kim H. Short-term outcomes of laparoscopic-assisted distal gastrectomy for gastric cancer during a surgeon’s learning curve period. Surg Endosc. 2009;23:2250–7.
Jung do H, Son SY, Park YS, et al. The learning curve associated with laparoscopic total gastrectomy. Gastric Cancer. 2016;19:264–72.
Kim MG, Kim KC, Yook JH, Kim BS, Kim TH, Kim BS. A practical way to overcome the learning period of laparoscopic gastrectomy for gastric cancer. Surg Endosc. 2011;25:3838–44.
Birkmeyer JD, Siewers AE, Finlayson EV, et al. Hospital volume and surgical mortality in the United States. N Engl J Med. 2002;346:1128–37.
Dikken JL, Verheij M, Cats A, Jansen EP, Hartgrink HH, van de Velde CJ. Extended lymph node dissection for gastric cancer from a European perspective. Gastric Cancer. 2011;14:396–8.
Kim MG, Kwon SJ. Comparison of the outcomes for laparoscopic gastrectomy performed by the same surgeon between a low-volume hospital and a high-volume center. Surg Endosc. 2014;28:1563–70.
Tokunaga M, Hiki N, Fukunaga T, et al. Learning curve of laparoscopy-assisted gastrectomy using a standardized surgical technique and an established educational system. Scand J Surg. 2011;100:86–91.
Yang SJ, Ahn EJ, Park SH, Kim JH, Park JM. The early experience of laparoscopy-assisted gastrectomy for gastric cancer at a low-volume center. J Gastric Cancer. 2010;10:241–6.
Murata A, Okamoto K, Muramatsu K, Matsuda S. Endoscopic submucosal dissection for gastric cancer: the influence of hospital volume on complications and length of stay. Surg Endosc. 2014;28:1298–306.
Ichikawa D, Komatsu S, Kubota T, et al. Effect of hospital volume on long-term outcomes of laparoscopic gastrectomy for clinical stage I gastric cancer. Anticancer Res. 2013;33:5165–70.
Kim TH, Kim JJ, Kim SH, et al. Diagnostic value of clinical T staging assessed by endoscopy and stomach protocol computed tomography in gastric cancer: the experience of a low-volume institute. J Gastric Cancer. 2012;12:223–31.
Clavien PA, Barkun J, de Oliveira ML, et al. The Clavien-Dindo classification of surgical complications: five-year experience. Ann Surg. 2009;250:187–96.
Brisinda G, Crocco A, Tomaiuolo P, Santullo F, Mazzari A, Vanella S. Extended or limited lymph node dissection? A gastric cancer surgical dilemma. Ann Surg. 2012;256:e30–1.
Sabesan A, Petrelli NJ, Bennett JJ. Outcomes of gastric cancer resections performed in a high volume community cancer center. Surg Oncol. 2015;24:16–20.
Dikken JL, Wouters MW, Lemmens VE, et al. Influence of hospital type on outcomes after oesophageal and gastric cancer surgery. Br J Surg. 2012;99:954–63.
Murata A, Muramatsu K, Ichimiya Y, Kubo T, Fujino Y, Matsuda S. Influence of hospital volume on outcomes of laparoscopic gastrectomy for gastric cancer in patients with comorbidity in Japan. Asian J Surg. 2015;38:33–9.
Liang Y, Wu L, Wang X, Ding X, Liang H. The positive impact of surgeon specialization on survival for gastric cancer patients after surgery with curative intent. Gastric Cancer. 2015;18:859–67.
Kim CY, Nam BH, Cho GS, et al. Learning curve for gastric cancer surgery based on actual survival. Gastric Cancer. 2016;19:631–8.
You YH, Kim YM, Ahn DH. Beginner surgeon’s initial experience with distal subtotal gastrectomy for gastric cancer using a minimally invasive approach. J Gastric Cancer. 2015;15:270–7.
Nunobe S, Hiki N, Tanimura S, Nohara K, Sano T, Yamaguchi T. The clinical safety of performing laparoscopic gastrectomy for gastric cancer by trainees after sufficient experience in assisting. World J Surg. 2013;37:424–9.
Kim MC, Kim W, Kim HH, et al. Risk factors associated with complication following laparoscopy-assisted gastrectomy for gastric cancer: a large-scale Korean multicenter study. Ann Surg Oncol. 2008;15:2692–700.
Fujisaki M, Shinohara T, Hanyu N, et al. Laparoscopic gastrectomy for gastric cancer in the elderly patients. Surg Endosc. 2016;30:1380–7.
Hur H, Xuan Y, Ahn CW, Cho YK, Han SU. Trends and outcomes of minimally invasive surgery for gastric cancer: 750 consecutive cases in seven years at a single center. Am J Surg. 2013;205:45–51.
Lee SE, Kim YW, Lee JH, et al. Developing an institutional protocol guideline for laparoscopy-assisted distal gastrectomy. Ann Surg Oncol. 2009;16:2231–6.
Woo J, Lee JH, Shim KN, Jung HK, Lee HM, Lee HK. Does the difference of invasiveness between totally laparoscopic distal gastrectomy and laparoscopy-assisted distal gastrectomy lead to a difference in early surgical outcomes? A prospective randomized trial. Ann Surg Oncol. 2015;22:1836–43.
Jeong O, Ryu SY, Choi WY, Piao Z, Park YK. Risk factors and learning curve associated with postoperative morbidity of laparoscopic total gastrectomy for gastric carcinoma. Ann Surg Oncol. 2014;21:2994–3001.
Kim HS, Kim SO, Kim BS. Use of a clinical pathway in laparoscopic gastrectomy for gastric cancer. World J Gastroenterol. 2015;21:13507–17.
So JB, Lim ZL, Lin HA, Ti TK. Reduction of hospital stay and cost after the implementation of a clinical pathway for radical gastrectomy for gastric cancer. Gastric Cancer. 2008;11:81–5.
Acknowledgements
Supported in part by Grants from the National Research Foundation of Korea (2012R1A1A1043576 and 2015R1A1A1A05028000) and the Catholic Medical Center Research Foundation made in the program year of 2015.
Disclosure
The authors declare no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Lee, H.H., Son, SY., Lee, J.H. et al. Surgeon’s Experience Overrides the Effect of Hospital Volume for Postoperative Outcomes of Laparoscopic Surgery in Gastric Cancer: Multi-institutional Study. Ann Surg Oncol 24, 1010–1017 (2017). https://doi.org/10.1245/s10434-016-5672-7
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1245/s10434-016-5672-7