
Abstract
Background
Randomized trials have not demonstrated a survival benefit for axillary dissection in the elderly, but the use of axillary staging for women 70 years of age and older remains controversial.
Methods
We utilized the National Cancer Data Base to study the use of axillary staging from 2004 to 2010 on 102,026 clinically node-negative and estrogen receptor-positive cases of pT1N0 tumors. Chi-square and logistic regression models were used to determine the trends and factors related to axillary staging.
Results
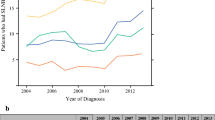
Axillary nodes were examined in 88.9 % of the total cohort, and the trend significantly increased from 87.7 % in 2004 to 89.2 % in 2010. A total of 77.2 % of patients underwent lumpectomy and 22.8 % mastectomy, with 87.0 % of lumpectomy patients undergoing axillary staging compared to 95.5 % of mastectomy patients. Predictors of axillary staging examined were age, comorbidity, income, histology, grade, facility type, facility location, and population density. The strongest independent predictor of axillary staging was age: 96.0 % of women aged 70–75 years underwent axillary staging, versus 92.3 % of women 75–80 years old, 83.2 % of women 80–85 years old, 66.5 % of women 86–90 years old, and 45.6 % of women >90 years old. Patients treated at academic/research facilities were 18.5 % less likely (odds ratio 0.81, 95 % confidence interval 0.76–0.87) than community cancer programs to undergo axillary staging. There was significant regional variation among U.S. Census regions: patients treated in the Midwest were 3.8 times more likely to undergo axillary staging than those treated in the Northeast.
Conclusions
Despite data indicating decreased utility, axillary staging remains overutilized in women with advancing age.




Similar content being viewed by others


References
Martelli G, Boracchi P, Ardoino I, et al. Axillary dissection versus no axillary dissection in older patients with T1N0 breast cancer: 15-year results of a randomized controlled trial. Ann Surg. 2012;256:920–4.
Rudenstam CM, Zahrieh D, Forbes JF, et al; International Breast Cancer Study Group. Randomized trial comparing axillary clearance versus no axillary clearance in older patients with breast cancer: first results of International Breast Cancer Study Group Trial 10-93. J Clin Oncol. 2006;24:337–44.
Hughes K, Schnaper LA, Berry D, et al. Lumpectomy plus tamoxifen with or without irradiation in women 70 years of age or older with early breast cancer. N Engl J Med. 2004;351:971–7.
Winchester DP, Stewart AK, Bura C, Jones RS. The National Cancer Data Base: a clinical surveillance and quality improvement tool. J Surg Oncol. 2004;85:1–3.
Bilimoria KY, Stewart AK, Winchester DP, Ko CY. The National Cancer Data Base: a powerful initiative to improve cancer care in the United States. Ann Surg Oncol. 2008;15:683–90.
American Cancer Society. Cancer facts and figures. http://www.cancer.org/Research/CancerFactsFigures/CancerFactsFigures/index. Accessed April 15, 2013.
Deyo RA, Cherkin DC, Ciol MA. Adapting a clinical comorbidity index for use with ICD-9-CM administrative databases. J Clin Epidemiol. 1992;44:613–9.
US Census Bureau. http://www.census.gov/main/www/cen2000.html. Accessed April 15, 2013.
Edge SB, Byrd DR, Compton CC, et al, eds. AJCC cancer staging manual. 7th ed. New York: Springer; 2010.
Percey CFA, Jack A. ICD-O: International classification of diseases for oncology. 3rd ed. Geneva: World Health Organization; 2000.
American College of Surgeons. Cancer programs. Categories of accreditation. http://www.facs.org/cancer/coc/categories.html. Accessed April 15, 2013.
US Census Bureau. Census regions and divisions of the United States. http://www.census.gov/main/www/cen2000.html. Accessed April 15, 2013.
Mansel RE, Fallowfield L, Kissin M, et al. Randomized multicenter trial of sentinel node biopsy versus standard axillary treatment in operable breast cancer: the ALMANAC trial. J Natl Cancer Inst. 2006;98:599–609.
Posther KE, McCall LM, Blumencranz PW, et al. Sentinel node skills verification and surgeon performance: data from a multicenter clinical trial for early-stage breast cancer. Ann Surg. 2005;242:593–9.
Sanghani M, Balk EM, Cady B. Impact of axillary lymph node dissection on breast cancer outcome in clinically node negative patients. Cancer. 2009;115:1613–20.
Fisher B, Jeong JH, Anderson S, Bryant J, Fisher ER, Wolmark N. Twenty-five-year follow-up of a randomized trial comparing radical mastectomy, total mastectomy, and total mastectomy followed by irradiation. N Engl J Med. 2002;347:567–75.
Early Breast Cancer Trialists’ Collaborative Goup (EBCTCG). Effect of chemotherapy and hormonal therapy for early breast cancer on recurrence and 15-year survival: an overview of the randomised trials. Lancet. 2005;365:1687–717.
Social Security Administration. Period life table, 2009. http://www.ssa.gov/oact/STATS/table4c6.html. Accessed April 15, 2013.
Conflict of interest
The authors declare no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Pesce, C., Czechura, T., Winchester, D.J. et al. Axillary Surgery Among Estrogen Receptor Positive Women 70 Years of Age or Older with Clinical Stage I Breast Cancer, 2004–2010: A Report from the National Cancer Data Base. Ann Surg Oncol 20, 3259–3265 (2013). https://doi.org/10.1245/s10434-013-3153-9
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1245/s10434-013-3153-9