
Abstract
Background
Completion lymph node dissection (CLND), although considered a standard approach for patients with melanoma and a positive sentinel lymph node (SLN), is not performed in as many as 50% of indicated cases. This study evaluates the outcome of patients who had a positive SLN but did not undergo CLND at Memorial Sloan-Kettering Cancer Center.
Methods
A prospective database was used to identify all patients with a positive SLN from 1992 to 2008. Patient and tumor characteristics, number of positive SLNs, recurrence pattern, reason for not performing a CLND, and current status were evaluated.
Results
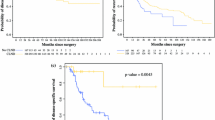
There were 2269 patients who underwent SLN biopsy. Three hundred thirteen had a positive SLN, of whom 271 (87%) had a CLND and 42 (13%) did not. Patients in the no-CLND group were older (median age 70 vs. 56 years, P < .01), and had a trend toward thicker melanomas (3.5 vs. 2.8 mm, P < .06). A significantly higher percentage of no-CLND patients had lower-extremity melanomas (40% vs. 13% CLND; P < .01). The most common reason for not performing a CLND was patient refusal (45%). There were similar rates and patterns of recurrence between the two groups. Recurrence-free survival and disease-specific survival were also similar between the groups.
Conclusions
It remains unclear whether CLND must be performed in all melanoma patients with a positive SLN. For selected informed patients who choose not to participate in the Multicenter Selective Lymphadenectomy Trial II trial, or in centers where the trial is not available, nodal observation may be an acceptable option.



Similar content being viewed by others


References
NCCN Practice Guidelines in Oncology: Melanoma. 2009;v.2.2009. www.nccn.org/index.asp.
Bilimoria KY, Balch CM, Bentrem DJ, et al. Complete lymph node dissection for sentinel node–positive melanoma: assessment of practice patterns in the United States. Ann Surg Oncol. 2008;15:1566–76.
Bilimoria KY, Stewart AK, Winchester DP, Ko CY. The National Cancer Data Base: a powerful initiative to improve cancer care in the United States. Ann Surg Oncol. 2008;15:683–90.
Cormier JN, Xing Y, Ding M, et al. Population-based assessment of surgical treatment trends for patients with melanoma in the era of sentinel lymph node biopsy. J Clin Oncol. 2005;23:6054–62.
Wrightson WR, Wong SL, Edwards MJ, et al. Complications associated with sentinel lymph node biopsy for melanoma. Ann Surg Oncol. 2003;10:676–80.
Wong SL, Morton DL, Thompson JF, et al. Melanoma patients with positive sentinel nodes who did not undergo completion lymphadenectomy: a multi-institutional study. Ann Surg Oncol. 2006;13:809–16.
Rosenberg SA. Why perform sentinel-lymph-node biopsy in patients with melanoma? (editorial). Nat Clin Pract Oncol. 2008;5:1.
Morton DL, Thompson JF, Cochran AJ, et al. Sentinel-node biopsy or nodal observation in melanoma. N Engl J Med. 2006;355:1307–17.
Gershenwald JE, Andtbacka RH, Prieto VG, et al. Microscopic tumor burden in sentinel lymph nodes predicts synchronous nonsentinel lymph node involvement in patients with melanoma. J Clin Oncol. 2008;26:4296–303.
Wrightson WR, Wong SL, Edwards MJ, et al. Reverse transcriptase-polymerase chain reaction (RT-PCR) analysis of nonsentinel nodes following completion lymphadenectomy for melanoma. J Surg Res. 2001;98:47–51.
Gershenwald JE, Berman RS, Porter G, Mansfield PF, Lee JE, Ross MI. Regional nodal basin control is not compromised by previous sentinel lymph node biopsy in patients with melanoma. Ann Surg Oncol. 2000;7:226–31.
Calabro A, Singletary SE, Balch CM. Patterns of relapse in 1001 consecutive patients with melanoma nodal metastases. Arch Surg. 1989;124:1051–5.
Pidhorecky I, Lee RJ, Proulx G, et al. Risk factors for nodal recurrence after lymphadenectomy for melanoma. Ann Surg Oncol. 2001;8:109–15.
Guggenheim MM, Hug U, Jung FJ, et al. Morbidity and recurrence after completion lymph node dissection following sentinel lymph node biopsy in cutaneous malignant melanoma. Ann Surg. 2008;247:687–93.
de Vries M, Vonkeman WG, van Ginkel RJ, Hoekstra HJ. Morbidity after inguinal sentinel lymph node biopsy and completion lymph node dissection in patients with cutaneous melanoma. Eur J Surg Oncol. 2006;32:785–9.
Cady B. Regional lymph node metastases; a singular manifestation of the process of clinical metastases in cancer: contemporary animal research and clinical reports suggest unifying concepts. Ann Surg Oncol. 2007;14:1790–800.
Ariyan C, Brady MS, Gonen M, Busam K, Coit D. Positive nonsentinel node status predicts mortality in patients with cutaneous melanoma. Ann Surg Oncol. 2009;16:186–90.
Chao C, Wong SL, Ross MI, et al. Patterns of early recurrence after sentinel lymph node biopsy for melanoma. Am J Surg. 2002;184:520–4.
Moore Dalal K, Zhou Q, Panageas KS, Brady MS, Jaques DP, Coit DG. Methods of detection of first recurrence in patients with stage I/II primary cutaneous melanoma after sentinel lymph node biopsy. Ann Surg Oncol. 2008;15:2206–14.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Kingham, T.P., Panageas, K.S., Ariyan, C.E. et al. Outcome of Patients with a Positive Sentinel Lymph Node who do not Undergo Completion Lymphadenectomy. Ann Surg Oncol 17, 514–520 (2010). https://doi.org/10.1245/s10434-009-0836-3
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1245/s10434-009-0836-3