
Abstract
Background:
Previous pooled analyses have reported an association between magnetic fields and childhood leukaemia. We present a pooled analysis based on primary data from studies on residential magnetic fields and childhood leukaemia published after 2000.
Methods:
Seven studies with a total of 10 865 cases and 12 853 controls were included. The main analysis focused on 24-h magnetic field measurements or calculated fields in residences.
Results:
In the combined results, risk increased with increase in exposure, but the estimates were imprecise. The odds ratios for exposure categories of 0.1–0.2 μT, 0.2–0.3 μT and ⩾0.3 μT, compared with <0.1 μT, were 1.07 (95% CI 0.81–1.41), 1.16 (0.69–1.93) and 1.44 (0.88–2.36), respectively. Without the most influential study from Brazil, the odds ratios increased somewhat. An increasing trend was also suggested by a nonparametric analysis conducted using a generalised additive model.
Conclusions:
Our results are in line with previous pooled analyses showing an association between magnetic fields and childhood leukaemia. Overall, the association is weaker in the most recently conducted studies, but these studies are small and lack methodological improvements needed to resolve the apparent association. We conclude that recent studies on magnetic fields and childhood leukaemia do not alter the previous assessment that magnetic fields are possibly carcinogenic.
Similar content being viewed by others

Main
Over the past three decades, potential health effects of residential and occupational exposure to extremely low-frequency electric and magnetic fields have been extensively investigated in epidemiological studies. Most attention has focused on a potential association between residential magnetic field exposure and childhood leukaemia. Almost all individual studies on magnetic fields and childhood leukaemia have found increased risks associated with the top percentiles of exposure levels; most of them, however, have involved a small number of exposed cases at the top percentiles. This has given rise to various interpretations. Two pooled analyses by Ahlbom et al, (2000) and Greenland et al, (2000), based on 9 and 12 studies, respectively, published up to 1999, have provided a basis for concluding that a consistent epidemiological association exists between residential exposure to magnetic fields and the risk of childhood leukaemia. Similar results were obtained by pooling data from four studies that included 24/48 h measurements, for exposure over the entire day and at night only (Schuz et al, 2007). Although hundreds of laboratory studies have been published, with a few reporting positive findings, most of the laboratory work has been negative. This has led to the general conclusion that robust, reliable and reproducible evidence of effects of magnetic fields at environmental levels on biological systems, either in vivo or in vitro, is lacking (IARC, 2002; WHO EHC, 2007). Thus, largely on the basis of epidemiological association of residential magnetic field exposure and childhood leukaemia, the International Agency for Research on Cancer has classified extremely low-frequency magnetic field exposure as being possibly carcinogenic to humans (Group 2B; IARC, 2002).
Since carrying out the pooled analyses, several new epidemiological studies have been published. The World Health Organization (WHO) reviewed results of the studies available through to 2006 in an Environmental Health Criteria (EHC) monograph (WHO EHC, 2007), with the conclusion that the ‘possibly carcinogenic’ classification does not change with the addition of new studies, but that the pooled analyses should be updated with the results from recent studies. In fact, such an analysis is identified as a high research priority in the WHO research agenda issued in 2007 (WHO, 2007).
We present a pooled analysis based on primary data of seven recent studies on magnetic fields and childhood leukaemia, to assess whether the combined results, adjusted for potential confounding, confirm the results of previous pooled analyses and whether there is an association between EMF exposure and childhood leukaemia.
Materials and Methods
Selection
We searched the published literature through PubMed, as well as references of identified papers, and conducted an informal survey of epidemiologists involved in magnetic field research to identify relevant recent and ongoing studies on residential magnetic field exposure and childhood leukaemia published since the previous pooled analyses of childhood leukaemia published in (Ahlbom et al, 2000; Greenland et al, 2000). To be included, studies had to provide data for children, provide data separately for leukaemia, be population based and provide measured or calculated residential magnetic fields inside a home. Studies that used distance to power lines as an exposure metric were also included, but not in the main analysis.
We identified 14 studies, of which seven met our inclusion criteria (Table 1). Appendix 1 summarises the methods and findings of studies that were not included. One study (Hoffmann et al, 2008) did not publish data on children and had a large overlap with a large countrywide German study (Schuz et al, 2001); to maintain independence of observations, only the countrywide German study (former West Germany) was included. Three studies were excluded because they were hospital based (Perez et al, 2005; Feizi and Arabi, 2007; Abdul Rahman et al, 2008). One study was excluded because it was a case-only study (Yang et al, 2008). Another study was excluded because it was exclusively of children with Down's syndrome, who are at substantially higher risk for leukaemia (Mejia-Arangure et al, 2007). One study, the Northern California Childhood Leukemia Study (NCCLS), was not made available in time for inclusion. However, the exposure assessment methods of this study were substantially different from all other measurement studies: a 30-min measurement was taken in the room with the median spot measurement after a survey of the entire residence, as compared with a 24-h or more measurement in the child's bedroom in all other measured field studies (Does et al, 2009). We attempted to obtain unpublished data from all known sources, and identified three additional studies that are underway, but with completion dates several years away.
Materials
One of the included studies (Brazil) has not yet been published (Wunsch Filho, personal communications, 2009). All included studies used a matched case–control design, although the matching variables were not the same in all studies (Bianchi et al, 2000; Schuz et al, 2001; Kabuto et al, 2006; Lowenthal et al, 2007; Kroll et al, 2010; Malagoli et al, 2010). In the original publication of one of the Italian studies, some of the controls were selected nonconcurrently (Bianchi et al, 2000). For this publication, the time period for that study was extended by 5 years by adding new cases and controls and was limited to the period for which concurrent control selection was possible (1978–1997). As we wanted to use as many cases and controls as possible to increase the flexibility of the analysis (and for other methodological reasons as described in Greenland et al, 2000), we ignored the matching and instead included adjustment for age of diagnosis, sex and study. To make the data as consistent as possible across studies, we limited the age of diagnosis to 0–15 years inclusive and converted all measured and calculated field from milligauss to microtesla. However, it should be noted that the Brazilian study included children of age 8 years or younger only, because computerised records of birth certificates used for control selection were available only from 2000 onwards. It is also the only study that includes only acute lymphoblastic leukaemia (ALL) cases.
We focused on surrogates of magnetic fields at home. All studies had long-term measurements (Brazil, Germany, Japan) or calculated magnetic fields (Italy1, Italy2, UK), except for the Tasmanian study, which included only distance to power lines. The long-term measurement studies used metres placed in the child's bedroom. Long-term measurements were taken for 24 h in two studies (Brazil, Germany), and for a 1-week period in one study (Japan). Long-term measurements can be affected by short-duration exposure to high fields, e.g., from domestic electrical appliances, which are not part of the background field at home. We followed Ahlbom et al (2000) and used geometric means of the long-term measurements in our analyses to reduce such effects. Three studies (UK, Italy1, Italy2) provided calculated fields, on the basis of distance between the subject's home and the closest line, taking into account historical load conditions and other line characteristics.
The studies provided exposure measurements for home at diagnosis (Brazil, Italy1, Japan), for birth home (UK) or for the home in which the child lived for the longest period of time before diagnosis (Germany). Two studies (Italy2, Tasmania) evaluated multiple residences. Some mechanisms of carcinogenesis could operate perinatally or antenatally, others later in life. In the absence of a known mechanism for magnetic fields, there is little basis for preferring one period over another, and the choice in individual studies has been highly influenced by practicalities of study design. To select an exposure proxy for subjects from these studies, we used the diagnosis home if available; if not, we used the home in which the subject lived the longest, and if that is not available, we used birth home, on the basis that, for measurement studies, more recent measurements are probably more reliable.
A number of potential confounders such as the type of dwelling, mobility, urbanisation, socioeconomic status (SES) and traffic exhaust were available in some studies (see Table 1). The number, type and coding of potential confounders differed among the studies. We examined mobility (dichotomised as one or more than one residence before diagnosis) and SES. Variables coding SES differed by study. We standardised SES to a three-level ordinal variable (low, medium and high) on the basis of SES in each country. Other potential confounders were available from too few studies to merit examination.
Statistical methods
The analysis plan largely followed that of the pooled analysis of Ahlbom et al (2000). An analysis using exposure as a linear predictor was conducted for a likelihood ratio test of homogeneity of effects across studies. In most analyses, increasing exposure categories of 0.1–<0.2 μT, 0.2–<0.3 μT and ⩾0.3 μT, with reference category <0.1 μT, were used. A highest cutoff point of 0.3 μT was chosen to obtain more stable results for the high-exposure category and to enable a direct comparison with results obtained by Greenland (Greenland et al, 2000). For comparison with results in Ahlbom, we also present some results with the highest cutoff point of 0.4 μT. Data were analysed using both ordinary logistic regression, with fixed intercepts to adjust for study, and mixed effects logistic regression, with random intercepts and exposure effect coefficients for study. Ordinary and mixed effects logistic regression yielded similar results; hence, we present results of the ordinary logistic regression analysis only. We also obtained odds ratios using a moving window of exposure. These analyses used exposure categories of 0.1–<0.2, 0.15–<0.25, 0.20–<0.30, 0.25–<0.35, ⩾0.30, ⩾0.35 and ⩾0.40, with reference category <0.1 μT, and were adjusted for age, sex and study. We estimated the trend in the log odds of being a case using a generalised additive model (GAM) (Hastie and Tibshirani, 1990) using a nonparametric curve (natural cubic smoothing spline with interior and boundary knots at the unique values of exposure) to estimate the risk associated with exposure, while controlling for study, age and sex. As a sensitivity analysis, we used a range of smoothing parameters (degrees of freedom, d.f.). These results were obtained using the gam package in R version 2.9.2 (R Development Core Team, 2009). Other analyses were conducted using Stata (StataCorp, 2007).
Results
Of the included studies, four were conducted in Europe, and one each was conducted in Japan, Brazil and Australia. Table 1 shows the numbers of cases and controls for each study, along with variables supplied by those studies. There was a total of 10 865 cases and 12 853 controls with exposure surrogates; however, total numbers in the high-exposure categories were small, even for this large data set.
Table 2 presents the absolute numbers of subjects by case–control status, study and exposure level. The UK study provided by far the largest number of cases and controls, i.e., 89 and 75%; however, influence on results is more dependent on the numbers in the high-exposure category, and thus Brazil with high numbers of exposed was expected to be the most influential. Overall, in the highest-exposure category (⩾0.3 μT), there were 26 cases and 50 controls, 11 and 30 of them from the study in Brazil. Four studies (Germany, Italy1, Italy2 and Japan) provided histological type of leukaemia. Among subjects with data on type of leukaemia available, 86% were ALL cases. Numbers for other subtypes were too low to support additional analysis by subtype.
Table 3 summarises the main results. We present results for geometric means for long-term measurements (results for arithmetic means were similar) for each study adjusted for basic potential confounders, and separately for measured and calculated field studies, as well as combined results. A likelihood ratio test comparing models with and without random effects for exposure did not detect heterogeneity (P=0.201), supporting the pooling of studies.
In most individual studies and in the combined results, the risk increased with increase in exposure, although the estimates were imprecise. For calculated field studies, the number of subjects in high-exposure categories was often too small to provide reliable estimates. As Brazil was the most influential study in terms of the number of highly exposed subjects, and included only young and only ALL cases, we present results with and without Brazil. Influence analysis omitting one study at a time confirmed that Brazil was the most influential study (results not shown). Without Brazil, the summary odds ratio for ⩾0.3 μT vs <0.1 μT is 1.56 (95% CI 0.78–3.10), which is close to the age, sex and study-adjusted summary OR of 1.68 (95% CI 1.23–2.31) obtained in the pooled analysis of Greenland (Greenland et al, 2000), but less precise. In individual studies and in combined results, the number of observed cases ⩾0.3 μT was higher than the expected number obtained by modelling the probability of membership in exposure categories on the basis of the distribution of controls, including covariates.
For a more direct comparison of the current pooled results with those of Ahlbom et al, we conducted an analysis using the same cutoff points. Our overall risk estimates, although compatible with previously reported estimates, are substantially lower (Table 4). This is particularly true for studies on measured fields, a result heavily influenced by the Brazilian study. The combined OR for ⩾0.4 μT vs <0.1 μT with Brazil omitted was 2.02 (95% CI 0.87–4.69), whereas combined ORs when omitting other single studies ranged from 1.32 to 1.49. When the Brazilian study is excluded from the analysis, our point estimates are very close to the results of Ahlbom et al. The same is true when a cutoff point ⩾0.3 μT is used, rather than ⩾0.4 μT.
Odds ratio estimates using categorical cutoff points and involving relatively small numbers of subjects are vulnerable to unstable results. To address this concern, we also calculated odds ratios using a moving window of exposure levels (Figure 1). These results also suggested a possible trend of increasing risk with increase in exposure; however, the estimates were imprecise.

Odds ratios (95% CI) for moving window of exposure levels, adjusted for age, sex, SES and study. Reference level: <0.1 μT.
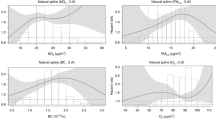
An ordinary logistic regression analysis using exposure as a continuous linear predictor yielded OR=1.11 (95% CI 0.98–1.26) for each increase of 0.2 μT, adjusting for age and sex. However, we prefer using a GAM, which is a more flexible modelling approach that provides a nonparametric estimate of the association between exposure and risk while controlling for potential confounders. Figure 2 presents the GAM nonparametric estimate of the trend in the log odds of being a case, with adjustment for study, age and sex. As a sensitivity analysis, we present results for a range of smoothing parameters, expressed as d.f., with models with more d.f. reflecting more fidelity to the data and models with fewer d.f. yielding more smoothing. Confidence limits widen as exposure increases, reflecting smaller number of subjects at high exposure levels. Although the curve suggests a positive exposure–response relationship, the width of the confidence bands indicates that a variety of exposure–response relationships, including no increase in risk, are compatible with the data.

Nonparametric estimates of trend in log odds of being a case with a range of levels of smoothing (A. 2 d.f.; B. 3 d.f.; C. 4 d.f.; D. 5 d.f.) from a generalised additive model, with adjustment for study, age of diagnosis and sex. Outer dotted lines represent 95% confidence limits.
Table 5 presents sensitivity and subgroup analyses in which we examine whether results change with adjustments for potential confounders and to what extent results are limited to a particular subgroup. Not all potential confounders were available in all studies. Analyses adjusting for confounding were carried out on the subset of studies and subjects for which data on the confounder were available. Most adjustments did not make appreciable changes in odds ratio estimates. Risks were a little higher for ALL and for a younger age group, and a little lower for residences at birth, despite a suggestion from one study (Lowenthal et al, 2007) that exposure at birth might carry particular risks. Neither an adjustment for mobility nor restriction to subjects who lived in a single residence before diagnosis changed the risk estimates appreciably. All confidence intervals included the null value.
In very early studies on magnetic field exposure, distance from power lines was used as a proxy for magnetic fields, but distance alone is a poor predictor of magnetic fields when a study involves lines of varying characteristics, as highlighted in a recent methodological paper (Maslanyj et al, 2009). Draper et al, (2005) found elevated risks at distances well beyond the point at which the magnetic fields from power lines would be elevated, but were unable to offer an explanation for this finding. Using the pooled data, we, similar to Draper et al (2005), evaluated the risk of childhood leukaemia as it relates to distance as an ‘exposure’ in its own right and not as a substitute for magnetic fields.
The results for risk of childhood leukaemia as related to distance based on six studies (all except Germany) are shown in Table 6. Risk estimates increase with a decrease in distance, and the risk estimate for the closest band (⩽50 m) is the highest and relatively precise, but full exploration of how this effect occurs will require consideration of the different voltage lines involved and the effect of alternative reference levels.
Discussion
We conducted a pooled analysis of seven recent epidemiological studies on the association between residential magnetic field exposure and childhood leukaemia. Pooled analysis, considered the gold standard for synthesising results from multiple studies, allows for comparison across different studies and metrics, free of artefacts introduced by analytical differences, and for derivation of statistically more stable results (Kheifets et al, 2006). Pooled analysis uses raw data from previous studies, and thus can apply identical analyses to all included studies. The choices of cutoff points, reference groups, metrics, etc., in a pooled analysis may differ from the choices made in the original studies and may result in changes in the study-specific effect estimates. Despite strengths, results from pooled analyses are prone to the same biases operating in the original studies. Studies using measurements generally have low participation rates, which might have led to selection bias (Mezei and Kheifets, 2006; Schuz and Ahlbom, 2008). Studies estimating calculated fields do not require participation and are thus less vulnerable to selection bias, but they neglect sources of magnetic fields other than high-voltage power lines and are thus likely to introduce exposure misclassification and loss of statistical power.
Our results, adjusting for potential confounding, broadly confirm the results of the previous pooled analyses by Greenland and Ahlbom, although the association is weaker when all studies are included. Our results are highly dependent on one study from Brazil that has greater influence because of comparatively high numbers of cases and controls at the upper exposure level. Possible explanations for the weaker association seen in the study from Brazil include: this study is affected by a bias that masks a true association more than other studies; this study is less affected by a bias evident in other studies that creates a spurious or stronger association; or that this is only a random variation.
Several unique features of the Brazilian study raise questions about the potential for bias. On one hand, it focuses on ALL, a more specific definition of disease, and on children <8 years of age, making it more likely that residential exposures are representative of total exposure. However, our subgroup analyses of ALL and of younger ages showed no strong indication that specificity of diagnosis or age is important. On the other hand, there are several limitations that might have led to bias. It is common in Brazil to move close to the treating hospital, and subjects who moved after diagnosis were not included, as it was logistically infeasible to conduct measurements in the homes in which they lived before diagnosis. In addition, participation between cases and controls was highly differential, in part because of the use of birth certificates as a source for controls and the difficulty in tracing individuals. As a result, 94.2% of controls in the Brazilian study have lived in a single residence, compared with 54.0% of cases. Thus, we speculate that the Brazilian study unduly pushes our risk estimates down. This is confirmed by an analysis of Brazilian data limited to residentially stable subjects: OR for ⩾0.3 μT vs <0.1 μT increases to 1.46 (95% CI 0.61–3.50, adjusted for age, sex and SES).
Although our results are compatible with no effect, when considering all studies combined, our findings suggest a small increase in risk with increasing exposure, regardless of the model chosen. Without the Brazilian study, our estimates are very close to those by Ahlbom et al, but less precise. Importantly, this pooled analysis, as compared with previous pooled analyses, includes a wider range of countries, including those in Asia and South America.
Most of the studies not included reported much higher estimates of risk, but had serious methodological problems. The addition of the one study that met our inclusion criteria but was not made available in time for this analysis, the Northern California Childhood Leukaemia Study, changes the risk estimates only slightly, resulting in OR=1.29 (0.81–2.06) for exposure ⩾0.3 μT (results obtained using counts of cases and controls in exposure categories for NCCL, which were available from the conference presentation; results adjusted for study only, as confounders were not available). Recall, however, that the measurements in this study are substantially different in length and most importantly in the location chosen for measurements.
In conclusion, our results are in line with previous pooled analyses showing an association between residential magnetic field exposure and childhood leukaemia, but the association is weaker in recent studies and imprecise because of small numbers of highly exposed individuals. At the same time, recent studies are small and lack methodological improvements needed to resolve scientific uncertainties regarding the apparent association. In the IARC classification scheme, a key issue is whether ‘chance, bias and confounding could be ruled out with reasonable confidence’. Our results, added to the previous pooled analyses, make chance less likely, but do not rule out bias or confounding, as whatever bias or confounding was present in previous studies could be present in these studies as well. Therefore, our results support conclusions of the WHO EHC (WHO EHC, 2007) and the European Union Scientific Committee on Emerging and Newly Identified Health Risks (Scientific Committee on Emerging and Newly Identified Health Risks, 2007) that recent studies on magnetic fields and childhood leukaemia do not alter the previous assessment that magnetic fields are possibly carcinogenic to humans.
Change history
29 March 2012
This paper was modified 12 months after initial publication to switch to Creative Commons licence terms, as noted at publication
References
Abdul Rahman HI, Shah SA, Alias H, Ibrahim HM (2008) A case-control study on the association between environmental factors and the occurrence of acute leukemia among children in Klang Valley, Malaysia. Asian Pac J Cancer Prev 9 (4): 649–652
Ahlbom A, Day N, Feychting M, Roman E, Skinner J, Dockerty J, Linet M, McBride M, Michaelis J, Tynes T, Verkasalo PK (2000) A pooled analysis of magnetic fields and childhood leukaemia. Br J Cancer 83 (5): 692–698
Bianchi N, Crosignani P, Rovelli A, Tittarelli A, Carnelli CA, Rossitto F, Vanelli U, Porro E, Berrino F (2000) Overhead electricity power lines and childhood leukemia: a registry-based, case-control study. Tumori 86 (3): 195–198
Does M, Scelo G, Metayer C, Selvin S, Kavet R, Buffler P (2009) Exposure to contact currents and magnetic fields and the risk of childhood leukemia. Paper presented at: The BIOEM 2009 Congress, Joint Meeting of The Bioelectromagnetics Society and the European BioElectromagnetics Association; 14-19 June, 2009; Davos, Switzerland
Draper G, Vincent T, Kroll ME, Swanson J (2005) Childhood cancer in relation to distance from high voltage power lines in England and Wales: a case-control study. BMJ 330 (7503): 1290
Feizi AA, Arabi MA (2007) Acute childhood leukemias and exposure to magnetic fields generated by high voltage overhead power lines – a risk factor in Iran. Asian Pac J Cancer Prev 8 (1): 69–72
Greenland S, Sheppard AR, Kaune WT, Poole C, Kelsh MA (2000) A pooled analysis of magnetic fields, wire codes, and childhood leukemia. Childhood Leukemia-EMF Study Group. Epidemiology 11 (6): 624–634
Hastie TJ, Tibshirani RJ (1990) Generalized Additive Models. Chapman and Hall/CRC: Boca Raton
Hoffmann W, Terschueren C, Heimpel H, Feller A, Butte W, Hostrup O, Richardson D, Greiser E (2008) Population-based research on occupational and environmental factors for leukemia and non-Hodgkin's lymphoma: the Northern Germany Leukemia and Lymphoma Study (NLL). Am J Ind Med 51 (4): 246–257
IARC working group (2002) Part 1: static and extremely low-frequency (ELF) electric and magnetic fields. IARC Monograph on the Evaluation of Carcinogenic Risks to Humans 80: 1–395
Kabuto M, Nitta H, Yamamoto S, Yamaguchi N, Akib S, Honda Y, Hagihara J, Isaka K, Saito T, Ojima T, Nakamura Y, Mizoue T, Ito S, Eboshida A, Yamazaki S, Sokejima S, Kurokawa Y, Kubo O (2006) Childhood leukemia and magnetic fields in Japan: a case-control study of childhood leukemia and residential power-frequency magnetic fields in Japan. Int J Cancer 119 (3): 643–650
Kheifets L, Mezei G, Greenland S (2006) Comment concerning ‘Childhood leukemia and residential magnetic fields: are pooled analyses more valid than the original studies?’ (Bioelectromagnetics 27:1-7 (2006)). Bioelectromagnetics 27 (8): 674–675; discussion 675–676
Kroll ME, Swanson J, Vincent TJ, Draper GJ (2010) Childhood cancer and magnetic fields from high voltage power lines in England and Wales: a case-control study. Br J Cancer (this issue)
Lowenthal RM, Tuck DM, Bray IC (2007) Residential exposure to electric power transmission lines and risk of lymphoproliferative and myeloproliferative disorders: a case-control study. Intern Med J 37 (9): 614–619
Malagoli C, Fabbi S, Teggi S, Calzari M, Poli M, Ballotti E, Notari B, Bruni M, Palazzi G, Paolucci P, Vinceti M (2010) Risk of hematological malignancies associated with magnetic fields exposure from power lines: a case-control study in two municipalities of northern Italy. Environ Health 9: 16
Maslanyj M, Simpson J, Roman E, Schuz J (2009) Power frequency magnetic fields and risk of childhood leukaemia: misclassification of exposure from the use of the ‘distance from power line’ exposure surrogate. Bioelectromagnetics 30 (3): 183–188
Mejia-Arangure JM, Fajardo-Gutierrez A, Perez-Saldivar ML, Gorodezky C, Martinez-Avalos A, Romero-Guzman L, Campo-Martinez MA, Flores-Lujano J, Salamanca-Gomez F, Velasquez-Perez L (2007) Magnetic fields and acute leukemia in children with Down syndrome. Epidemiology 18 (1): 158–161
Mezei G, Kheifets L (2006) Selection bias and its implications for case-control studies: a case study of magnetic field exposure and childhood leukaemia. Int J Epidemiol 35 (2): 397–406
Perez CB, Pineiro RG, Diaz NT (2005) Campos electromagneticos de baja frecuencia y leucemia infantil en Cuidad de La Habana. Rev Cubana Hig Epidemiol 43 (3): 1–10
R Development Core Team (2009) R: A Language and Environment for Statistical Computing [Computer Program]. Version 2.9.2. R Foundation for Statistical Computing: Vienna, Austria, URL http://www.R-project.org
Schuz J, Ahlbom A (2008) Exposure to electromagnetic fields and the risk of childhood leukaemia: a review. Radiat Prot Dosimetry 132 (2): 202–211
Schuz J, Grigat JP, Brinkmann K, Michaelis J (2001) Residential magnetic fields as a risk factor for childhood acute leukaemia: results from a German population-based case-control study. Int J Cancer 91 (5): 728–735
Schuz J, Svendsen AL, Linet MS, Linet MS, McBride ML, Roman E, Feychting M, Kheifets L, Lightfoot T, Mezei G, Simpson J, Ahlbom A (2007) Nighttime exposure to electromagnetic fields and childhood leukemia: an extended pooled analysis. Am J Epidemiol 166 (3): 263–269
Scientific Committee on Emerging and Newly Identified Health Risks (2007) Possible effects of electromagnetic fields on human health
StataCorp (2007) Stata Statistical Software: Release 10 (computer program). Version Release 10. StataCorp LP: College Station, TX
World Health Organization (2007) WHO Research Agenda for Extremely Low Frequency Fields. http://www.who.int/peh-emf/research/elf_research_agenda_2007.pdf. . Accessed Nov.1, 2009
World Health Organization Environmental Health Criteria (WHO EHC) (2007) Extremely Low Frequency Fields, Vol 238. WHO: Spain
Yang Y, Jin X, Yan C, Tian Y, Tang J, Shen X (2008) Case-only study of interactions between DNA repair genes (hMLH1, APEX1, MGMT, XRCC1 and XPD) and low-frequency electromagnetic fields in childhood acute leukemia. Leuk Lymphoma 49 (12): 2344–2350
Acknowledgements
This work was supported by funding from CHILDREN with LEUKAEMIA, a UK charity. CMC was also supported by NIH NCI CA016042. The Brazilian study was conducted under the EMF Project-SP, P&D project, with resources allocated by the Brazilian Electricity Regulatory Agency (0390-041/2004 ANNEL), coordinated by the Brazilian Association for Electromagnetic Compatibility (ABRICEM), and performed at the University of Sao Paulo School of Public Health. Main collaborators were Daniele M Pelissari, Dr Claúdia T de Oliveira, Dr Juliana F da Mata, Luiz G Tone, Dr Maria Lydia M de André, Dr Maria L Lee, Dr Paula Bruniera, Dr Sidnei Epelman and Dr Vicente Odone Filho. The Italy1 study was conducted by the National Cancer Institute of Milan, in collaboration with Health Local Unit (ASL) of Varese Province and of Regional Environmental Protection Agency (ARPA – Varese Province). The main collaborators were Crosignani P, Borgini A, Bertoldi M, Codazzi T, Bianchi N, Rovelli A and Porro E. The Italy2 study was supported by ASEOP (Associazione Sostegno Ematologia Oncologia Pediatrica) of Modena and by the Reggio Emilia Municipality – Department of the Environment. The main collaborators were Carlotta Malagoli MD, Mariagiulia Calzari PhD, Sara Fabbi PhD, Sergio Teggi PhD, Giovanni Palazzi MD, Paolo Paolucci MD, Maurizio Poli PhD, Elena Ballotti, Barbara Notari PhD and Maurizio Bruni. The German study was funded by the Federal Ministry for the Environment, Nuclear Safety and Nature Preservation, and we thank Drs Jörg Michaelis and Peter Kaatsch for providing the German data. RML sincerely thanks his co-workers on the Tasmanian study, Ms Deirdre Tuck (research associate) and Dr Issy Bray (statistician). We are grateful to Tim Vincent of the CCRG for his work on data from the UK study. JS worked on this paper with permission from the National Grid, but no results were shared nor was approval sought from anyone in the National Grid and the views expressed are his alone.
Author information
Authors and Affiliations
Corresponding author
Appendix 1
Appendix 1
Summary of recent studies not included in the pooled analysis
Rights and permissions
From twelve months after its original publication, this work is licensed under the Creative Commons Attribution-NonCommercial-Share Alike 3.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-sa/3.0/
About this article
Cite this article
Kheifets, L., Ahlbom, A., Crespi, C. et al. Pooled analysis of recent studies on magnetic fields and childhood leukaemia. Br J Cancer 103, 1128–1135 (2010). https://doi.org/10.1038/sj.bjc.6605838
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.bjc.6605838
Keywords
This article is cited by
-
Effect of Occupational Extremely Low-Frequency Electromagnetic Field Exposure on the Thyroid Gland of Workers: A Prospective Study
Current Medical Science (2022)
-
The Response of Osteoblasts and Bone to Sinusoidal Electromagnetic Fields: Insights from the Literature
Calcified Tissue International (2019)
-
Pulsed electromagnetic fields: promising treatment for osteoporosis
Osteoporosis International (2019)
-
Proximity to overhead power lines and childhood leukaemia: an international pooled analysis
British Journal of Cancer (2018)
-
Residential magnetic fields exposure and childhood leukemia: a population-based case–control study in California
Cancer Causes & Control (2017)
