
Abstract
Background
Robotic surgery has advantages to perform rectal cancer by its ergonomic designs and advanced technologies. However, it was uncertain whether these core robotic technologies could shorten the learning curve. The aim of this study is to investigate the learning curve of robotic rectal cancer surgery and to compare the learning curve phases with respect to perioperative clinicopathologic outcomes.
Methods
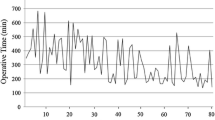
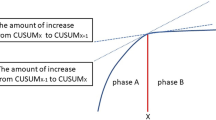
From April 2006 to August 2011, a total of 130 consecutive patients who were diagnosed with rectal cancer underwent a robotic low anterior resection (LAR) using the hybrid technique by a single surgeon at Severance Hospital. The moving average method and the cumulative sum (CUSUM) were used to analyze the learning curve. The risk-adjusted CUSUM (RA-CUSUM) analysis was used to evaluate the points, which showed completion of surgical procedures in terms of R1 resection, conversion, postoperative complications, harvested lymph nodes less than 12, and local recurrence. Perioperative clinical outcomes and pathologic results were compared among the learning curve phases.
Results
According to the CUSUM, the learning curve was divided into three phases: phase 1 [the initial learning period (1st–44th case), n = 44], phase 2 [the competent period (45th–78th case), n = 34], and phase 3 [the challenging period (79th–130th case), n = 52]. RA-CUSUM showed the minimum value at the 75th case, which suggested technical competence to satisfy feasible perioperative outcomes. The total operation time tended to decrease after phase 1 and so did the surgeon console time and docking time. Postoperative complications and pathologic outcomes were not significantly different among the learning phases.
Conclusions
The learning curve of robotic LAR consisted of three phases. The primary technical competence was achieved at phase 1 of the 44th case according to the CUSUM. The technical completion to assure feasible perioperative outcomes was achieved at phase 2 at the 75th case by the RA-CUSUM method.




Similar content being viewed by others
References
Jayne DG, Thorpe HC, Copeland J, Quirke P, Brown JM, Guillou PJ (2010) Five-year follow-up of the Medical Research Council CLASICC trial of laparoscopically assisted versus open surgery for colorectal cancer. Br J Surg 97:1638–1645
Green BL, Marshall HC, Collinson F, Quirke P, Guillou P, Jayne DG, Brown JM (2013) Long-term follow-up of the Medical Research Council CLASICC trial of conventional versus laparoscopically assisted resection in colorectal cancer. Br J Surg 100:75–82
Group TCOoSTS (2004) A comparison of laparoscopically assisted and open colectomy for colon cancer. N Engl J Med 350:2050–2059
Ballantyne GHMP, Wasielewski A, Weber A (2001) Robotic solutions to the pitfalls of laparoscopic colectomy. Osp Ital Chir 7:405–412
Bianchi PP, Ceriani C, Locatelli A, Spinoglio G, Zampino MG, Sonzogni A, Crosta C, Andreoni B (2010) Robotic versus laparoscopic total mesorectal excision for rectal cancer: a comparative analysis of oncological safety and short-term outcomes. Surg Endosc 24:2888–2894
Baik SH, Kwon HY, Kim JS, Hur H, Sohn SK, Cho CH, Kim H (2009) Robotic versus laparoscopic low anterior resection of rectal cancer: short-term outcome of a prospective comparative study. Ann Surg Oncol 16:1480–1487
Kwak JM, Kim SH, Kim J, Son DN, Baek SJ, Cho JS (2011) Robotic vs laparoscopic resection of rectal cancer: short-term outcomes of a case-control study. Dis Colon Rectum 54:151–156
Bokhari MB, Patel CB, Ramos-Valadez DI, Ragupathi M, Haas EM (2011) Learning curve for robotic-assisted laparoscopic colorectal surgery. Surg Endosc 25:855–860
Jimenez-Rodriguez RM, Diaz-Pavon JM, de Juan FDL, Prendes-Sillero E, Dussort HC, Padillo J (2013) Learning curve for robotic-assisted laparoscopic rectal cancer surgery. Int J Colorectal Dis 28:815–821
Akmal Y, Baek JH, McKenzie S, Garcia-Aguilar J, Pigazzi A (2012) Robot-assisted total mesorectal excision: is there a learning curve? Surg Endosc 26:2471–2476
D’Annibale A, Pernazza G, Monsellato I, Pende V, Lucandri G, Mazzocchi P, Alfano G (2013) Total mesorectal excision: a comparison of oncological and functional outcomes between robotic and laparoscopic surgery for rectal cancer. Surg Endosc 27:1887–1895
Sng KK, Hara M, Shin JW, Yoo BE, Yang KS, Kim SH (2013) The multiphasic learning curve for robot-assisted rectal surgery. Surg Endosc 9:3297–3307
Tekkis PP, Senagore AJ, Delaney CP, Fazio VW (2005) Evaluation of the learning curve in laparoscopic colorectal surgery: comparison of right-sided and left-sided resections. Ann Surg 242:83–91
Baik SH, Lee WJ, Rha KH, Kim NK, Sohn SK, Chi HS, Cho CH, Lee SK, Cheon JH, Ahn JB, Kim WH (2008) Robotic total mesorectal excision for rectal cancer using four robotic arms. Surg Endosc 22:792–797
Dindo D, Demartines N, Clavien PA (2004) Classification of surgical complications: a new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann Surg 240:205–213
Edge S, Byrd DR, Compton CC, Fritz AG, Greene FL, Trotti A (eds) (2010) AJCC cancer staging manual, 7th edn. Springer, New York
Adam IJ, Mohamdee MO, Martin IG, Scott N, Finan PJ, Johnston D, Dixon MF, Quirke P (1994) Role of circumferential margin involvement in the local recurrence of rectal cancer. Lancet 344:707–711
Baik SH, Ko YT, Kang CM, Lee WJ, Kim NK, Sohn SK, Chi HS, Cho CH (2008) Robotic tumor-specific mesorectal excision of rectal cancer: short-term outcome of a pilot randomized trial. Surg Endosc 22:1601–1608
Steiner SH, Cook RJ, Farewell VT, Treasure T (2000) Monitoring surgical performance using risk-adjusted cumulative sum charts. Biostatistics 1:441–452
Tekkis PP, Fazio VW, Lavery IC, Remzi FH, Senagore AJ, Wu JS, Strong SA, Poloneicki JD, Hull TL, Church JM (2005) Evaluation of the learning curve in ileal pouch-anal anastomosis surgery. Ann Surg 241:262–268
Cook DA, Duke G, Hart GK, Pilcher D, Mullany D (2008) Review of the application of risk-adjusted charts to analyse mortality outcomes in critical care. Crit Care Resusc 10:239–251
Son GM, Kim JG, Lee JC, Suh YJ, Cho HM, Lee YS, Lee IK, Chun CS (2010) Multidimensional analysis of the learning curve for laparoscopic rectal cancer surgery. J Laparoendosc Adv Surg Tech A 20:609–617
Schlachta CM, Mamazza J, Seshadri PA, Cadeddu M, Gregoire R, Poulin EC (2001) Defining a learning curve for laparoscopic colorectal resections. Dis Colon Rectum 44:217–222
Kayano H, Okuda J, Tanaka K, Kondo K, Tanigawa N (2011) Evaluation of the learning curve in laparoscopic low anterior resection for rectal cancer. Surg Endosc 25:2972–2979
Ito M, Sugito M, Kobayashi A, Nishizawa Y, Tsunoda Y, Saito N (2009) Influence of learning curve on short-term results after laparoscopic resection for rectal cancer. Surg Engosc 23:403–408
Akiyoshi T, Kuroyanagi H, Ueno M, Oya M, Fujimoto Y, Konishi T, Yamaguchi T (2011) Learning curve for standardized laparoscopic surgery for colorectal cancer under supervision: a single-center experience. Surg Endosc 25:1409–1414
Baik SH, Kim NK, Lim DR, Hur H, Min BS, Lee KY (2013) Oncologic outcomes and perioperative clinicopathologic results after robot-assisted tumor-specific mesorectal excision for rectal cancer. Ann Surg Oncol 20:2625–2632
Acknowledgments
The authors thank MiSun Park for the English revision of this manuscript.
Disclosures
Eun Jung Park, Chang Woo Kim, Min Soo Cho, Seung Hyuk Baik, Dong Wook Kim, Byung Soh Min, Kang Young Lee, Nam Kyu Kim have no conflicts of interest or financial ties of disclosure.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Park, E.J., Kim, C.W., Cho, M.S. et al. Multidimensional analyses of the learning curve of robotic low anterior resection for rectal cancer: 3-phase learning process comparison. Surg Endosc 28, 2821–2831 (2014). https://doi.org/10.1007/s00464-014-3569-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-014-3569-8