
Abstract
Background: Classic teaching has advocated the use of open biopsy to diagnose and grade extremity soft-tissue sarcoma. Reported advantages of core needle biopsy include the minimal morbidity, cost, and time. The perceived disadvantage has been diagnostic inaccuracy. The objective of this study was to compare the diagnostic accuracy of core needle biopsy to incisional or frozen section biopsy for primary extremity masses suspicious for soft-tissue sarcoma.
Methods: Patients presenting with extremity masses were identified from our prospective soft-tissue sarcoma database (malignant) and from the clinical information center (benign) between January 1, 1990, and December 31, 1995. Biopsy and subsequent resection data were collected from the pathologic records.
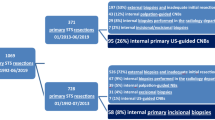
Results: During this time, 164 primary extremity soft-tissue masses were evaluated before any biopsy. As the initial diagnostic approach, there were 60 core needle, 44 incisional, 36 frozen section, and 26 excisional biopsies. Two patients underwent two biopsy procedures. Ninety-three percent of the specimens obtained at core needle biopsy were adequate to make a diagnosis. Of the adequate core needle biopsy specimens, 95%, 88% and 75% correlated with the final resection diagnosis for malignancy, grade, and histologic subtype, respectively. Of the frozen section biopsy specimens, 94% were adequate, and accurate diagnostic results of malignancy were obtained with 88%. However, only 62% and 47% were correct for grade and histologic subtype, respectively, which was significantly different than the results obtained with incisional biopsy. The false-negative and false-positive rates for core needle biopsy were 5% and 0% for malignancy. Two core needle biopsy specimens graded low were found to be high, and one core needle biopsy specimen graded high was subsequently found to be low on final resection.
Conclusions: When read by an experienced pathologist, the results of core needle biopsy provide accurate diagnostic information for malignancy and grade. Adequate core needle biopsy obviates the need for open biopsy and can be used for rational treatment planning. In the absence of adequate tissue, open biopsy is required.
Similar content being viewed by others


References
Brennan MF. Current management of soft tissue sarcoma.Ann Surg 1993;217:ii-v.
Shives TC. Biopsy of soft-tissue tumors [Review].Clin Orthop 1993;289:32–5.
Simon MA. Biopsy of musculoskeletal tumors.J Bone Joint Surg [Am] 1982;64:1253–7.
Brennan MF, Hilaris B, Shiu MH, Lane J, Magill G, Friedrich C, Hajdu SI. Local recurrence in adult soft-tissue sarcoma. A randomized trial of brachytherapy.Arch Surg 1987;122:1289–93.
Mankin HJ, Lange TA, Spanier SS. The hazards of biopsy in patients with malignant primary bone and soft-tissue tumors.J Bone Joint Surg [Am] 1982;64:1121–7.
Kissin MW, Fisher C, Carter RL, Horton LW, Westbury G. Value of Tru-Cut biopsy in the diagnosis of soft tissue tumours.Br J Surg 1986;73:742–4.
Ball AB, Fisher C, Pittam M, Watkins RM, Westbury G. Diagnosis of soft tissue tumours by Tru-Cut biopsy.Br J Surg 1990;77:756–8.
Barth RJ, Merino MJ, Solomon D, Yang JC, Baker AR. A prospective study of the value of core needle biopsy and fine needle aspiration in the diagnosis of soft tissue masses.Surgery 1992;112:536–43.
Heslin MJ, Woodruff JM, Brennan MF. Prognostic significance of a positive microscopic margin in high risk soft tissue sarcoma: Implications for management.J Clin Oncol 1996;14:473–9.
Moore TM, Meyers MH, Patzakis MJ, Terry R, Harvey JP Jr. Closed biopsy of musculoskeletal lesions.J Bone Joint Surg [Am] 1979;61:375–80.
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Heslin, M.J., Lewis, J.J., Woodruff, J.M. et al. Core needle biopsy for diagnosis of extremity soft tissue sarcoma. Annals of Surgical Oncology 4, 425–431 (1997). https://doi.org/10.1007/BF02305557
Received:
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/BF02305557